by Nutrilicious | Apr 16, 2019 | The Nation’s Health, Changing mindset, Impactful health initiatives
We’re excited to be involved in a new initiative to help tackle the critical problem of poor diet amongst lower income households: Shop Well – Eat Well. It’s a collaboration between the British Dietetic Association (BDA), Alpro and the Southwark Hub, with the aim of a multi-angled approach to have a real and lasting impact.
Launched last month, we brought together experts to give their insights into key topics. Here’s a summary of some of the key points, followed by links to each of the presentations, which we highly recommend you take the time to watch!
People on lower incomes have a worse diet and shorter life expectancy
There is a direct correlation between diet and income, in turn affecting health. The lower your income, the more likely it is you will:
- Eat more sugar, processed foods, fat and sodium
- Eat less fibre, vitamin A and folate
- Be less likely to meet iron, folate and calcium recommendations
- Eat less oil-rich fish
- Eat more take-aways
- Cook less at home from scratch
People in lower income groups in the UK have a significantly shorter life expectancy than the average: by nine years for women and seven for men.
They have double the rates of cardiovascular disease, lifestyle-related cancers, type 2 diabetes and total mortality compared to the national average. Obesity prevalence of the most deprived 10% of children is approximately twice that of the least deprived 10%.
This is not new news. Countless attempts have been made to try to address the problem and encourage people on lower incomes to eat more healthily, thereby increasing their quality of life and life expectancy.
But when it comes to eating habits, behaviour change is very difficult to achieve.
Barriers to healthy eating are multiple, complex and interlinked – psychological, financial, environmental, conscious and unconscious. Among lower income households they include:
- Financial barriers – For low income families, a big barrier to buying new foods or going to a new food shop is not knowing how much the food will cost, or assuming that it will all be expensive. Parents want to know exactly how much their shopping basket is before they reach the checkout.
- Social barriers – Food habits get passed down the generations as young people grow up and become parents themselves. What children see their parents and families doing is what they grow up thinking of as ‘normal’.
- Preparation space – Cooking from scratch relies on kitchen equipment, confidence in cooking skills, time to prepare food and pleasant surroundings – not the case for many on low income.
- Limited bandwidth – The cognitive burden of living under financial strain and other modern day life stresses reduce parents‘ mental bandwidth; brainpower that would otherwise go to planning ahead and problem-solving.[1] Families in this situation look for quick and easy ways to eat, and takeaway and convenience foods provide an in-the-moment solution to feeding children quickly, affordably and safely.
- Advertising and shop layouts – Cues such as special offers, advertising for takeaways, attractive packaging and child-height shelving nudge families towards less healthy foods in shops.
- It’s not always a lack of knowledge or cost that’s a problem, it’s translating knowledge to practice.
In fact, most eating behaviour is driven by unconscious, habitual processes. These are largely immune to education when it comes to behaviour change. Yet this has been our predominant approach to changing dietary behaviour!
Breaking the habits of a lifetime
Multiple collaborative strategies are needed to succeed in changing behaviour: from government, local authority, industry and all food providers, alongside continuing to help individuals overcome their personal barriers.
We need to making healthy eating
- easy,
- habitual, and
- normal
As behavioural psychologist Dr. Paul Chadwick says, it’s not sustainable for people to have to think about every food choice that they make. Healthy eating has to become the default option.
A new initiative for change
Behavioural science shows the importance of interactions between the individual and their physical and social environment when it comes to habit forming and breaking.
It’s time the food environment changed to make healthy eating as easy to attain as possible for all, including low affluent groups.
It’s also time for families and individuals to be supported in overcoming barriers to breaking the unhealthy habits.
 We’re excited to be part of the new initiative, Shop Well – Eat Well, to help enable this – especially targeting those on a low income.
We’re excited to be part of the new initiative, Shop Well – Eat Well, to help enable this – especially targeting those on a low income.
Starting as a year-long pilot in Southwark, South London, it’s kicking off in June. Community charities and volunteers will join to create peer and professional-led healthy eating seminars and workshops tailored to the young, old and families.
At the launch, Kate Arthur, UK External Scientific Affairs & Nutrition Manager at Alpro, explained: “We wanted to find interventions that would encourage people to think about their food choices differently.
“Going directly into the community to find out what will work for people is the logical thing to do. We’ll be working on different engaging activities such peer led cookery workshops and drop in seminars, with help from the BDA Let’s get Cooking and an advisory committee of experts, always with an eye on the main barriers.
“Ultimately, we’ll be assessing to see what really makes a difference over the next year of the campaign and we’ll share any success stories widely with local communities nationwide and the dietetic community as a whole.”
Caroline Bovey, Chair of the British Dietetic Association added: “By partnering on this project, and working with the food manufacturers and shops that people are accessing daily, we’re excited to directly tackle some of the wider barriers to healthy habits in a local area. The BDA is delighted to be working with Alpro and the Southwark wellbeing hub to help people who often have to prioritise the other demands of daily life over their food choices.”
Take advantage of insightful presentations and useful resources
At our launch, five leading experts presented the latest evidence and initiatives to help overcome barriers to healthy shopping baskets and healthy eating. The presentations are available on the Shop Well – Eat Well website. Make yourself a cup of tea, watch, learn and be inspired:
– Dr Paul Chadwick, behaviour change leading expert: A scientific approach to behaviour change
– Sue Baic, Registered Dietitian: Affordable, healthy and sustainable eating in practice
– Duncan Brown, Development Director at charity Shift design: How does affluence impact on food choices?
– Kate Arthur, Alpro UK’s External Scientific Affairs & Nutrition Manager: Changing behaviour in the community
– Nilani Sritharan, Company Nutritionist at Sainsbury’s Supermarkets Ltd: Making healthy shopping easier
You’ll also find practical and engaging resources to help consumers overcome their barriers to healthy eating.
#shopwelleatwell @SouthwarkHub @BDA_Dietitians @Alpro
by Tanya HAFFNER | Jan 25, 2019 | Hot Topics in nutrition, Surveys and insights
“The world’s diets must change dramatically,” said Harvard University’s Walter Willett, one of the leaders of the comprehensive EAT-Lancet report released this week researching healthy and sustainable diet.
The findings show we must drastically cut down on meat and dairy, and eat more plant foods.
Published after three years of reviewing extensive evidence from around the world, the message is similar to that of both the British Dietetic Association’s One Blue Dot campaign, the government Eatwell Guide, the World Health Organisation and recommendations made by various non-governmental health organisations, for example World Cancer Research Fund (WCRF) and the British Heart Foundation.
The EAT-Lancet recommended daily diet
Here’s an outline of the recommended daily diet to meet 2,500kcal and all micronutrients:
|
Average recommended intake* |
Comment
|
| Daily |
Weekly |
| Protein foods |
| Beef, lamb and pork |
14g |
98g |
· Less than a quarter pounder per week
· Significantly below the WCRF recommendations of 350-500g per week
· 70-90% below current US & European intakes |
| Chicken and other poultry |
29g |
203g |
· Equivalent to around 1½ chicken breasts per week
· EAT suggests that the poultry allowance can be exchanged for eggs, fish or plant proteins and vice versa |
| Eggs |
13g |
91g |
· Equivalent to around 1½ eggs per week |
| Fish |
28g |
196g |
· Around 1½ – 2 servings a week
· Oil rich fish is strongly recommended as an omega-3 source |
| Legumes: dry lentils, beans, peas & soya foods |
75g |
525g |
· Equivalent to roughly 150g cooked / tinned beans daily
· An allowance within the 75g recommendation for soya products is specified due to the association with lower breast cancer incidence and reduced cholesterol levels |
| Tree nuts & peanuts |
50g |
350g |
· Equivalent to 1½ handfuls daily
· The report acknowledges that some nut and legume crops use intense water farming. However, the evidence for their associated reduced cardiovascular disease, cancer and total mortality risk justified this environmental trade off. |
| Dairy |
| Milk or equivalent in cheese / yogurt etc. |
250g |
1.75L |
· This is a significant reduction in dairy recommendations |
| Carbohydrates |
| Rice, wheat, corn and other, dry weight |
232g |
1.62kg |
· Whole grains advocated
· Equivalent to 1 servings of rice or pasta, 40g serving of breakfast cereals & 2 large slices bread daily |
| Tubers or starchy vegetables |
50g |
350g |
· Equivalent to 1 egg-sized potato daily or 1½ baked potatoes weekly |
| Non-starchy vegetables |
| All vegetables |
300g |
2.1kg |
· Notably, more vegetables than fruit recommended
· 3-4 servings daily |
| All fruits |
200g |
1.4kg |
· 2 servings daily |
| Added fats |
| Unsaturated oils |
40g |
280g |
· Equivalent to 4tbsp oil daily |
| Saturated oils |
≤11.8g |
≤83g |
· An allowance was made taking into consideration using all animal parts
· Equivalent to a single butter pack |
| Added sugars – no more than 5% energy intake – approx. 30g or 7tsp per adult per day. |
* EAT-Lancet recommended diet as well as an average daily intake, also provides a range of intakes.
Some of the notable findings are around red meat for iron and dairy for calcium:
- Iron: There is a problem with deficiency for adolescents but encourages use of inexpensive supplements over consumption of red meat
- Calcium: The United States and other countries over-estimate calcium needs. It is ubiquitous in the diet and there is little evidence that intakes above 500mg per day improve bone health.
The report looks how to change people’s choices to include less meat/dairy, through:
– making healthier foods more accessible and more cost effective
– reducing marketing and availability of unhealthy food.
It also tackles farming changes to a high degree – seen as being as important as, if not more than consumer change.
Conclusion? Change is needed, it’s going to be tough
We need to make big changes in our eating patterns if we’re going to protect our planet and health. It requires a multi-system combined effort approach to reduce food waste/losses, improve food production and encourage dietary shifts.
It is time for everyone to be involved in the urgently-needed transformation of our food system. We’ll be monitoring the impact the report has over time. Stay tuned…
by Tanya HAFFNER | Jan 17, 2019 | Hot Topics in nutrition, The Nation’s Health
What’s hot in the wacky world of wellness in 2019
Historians believe that the practice of New Year resolutions originated in the Babylonian Kingdom, over 3,000 years ago. New Year intuitively brings time for pause, reflection and setting intentions for the year, and for many, that can centre on resetting what they eat, especially after indulging over the holidays.
In their annual round-up of the more bizarre fad diets for 2019, the BDA have suggested that the blood type diet, drinking your own pee (yes, really), detox teas/skinny coffee, slimming sachets and alkaline water, are some of the more bizarre regimes they’re coming up against.
Here’s a look at what else is hot in the wellness space, with some links to relevant, recent research that may help you in your daily communications or practice.
Lasting fasting
One thing that has remained popular as we come into the New Year, has been the idea of fasting and this month, Jurassic World actor Chris Pratt, announced to his 22.2 million followers that he’s doing the Daniel Fast.
If you haven’t heard of it, the Daniel Fast was created over a decade ago by Susan Gregory, according to the website, a ‘lay minister, businesswoman, coach for Christian living and wannabe techie’ and is a 21-day period of prayer and partial fasting practised by some Christians, based on the experience of the Prophet Daniel’s and Jewish fasting principles. According to the website, the permitted foods centre around vegan options, with some additional restrictions including all sweeteners (non-nutritive and nutritive), processed foods and solid fats.
Elsewhere and currently number 2 on Amazon.co.uk’s bestseller list for diet books, is Michael Mosley’s ‘The Fast 800’ (in fact it appears twice in the top-10 as a hardback and paperback). His latest offering since the popular 5:2 diet and 8-week Blood Sugar Diet (also still in the top-20), which centres on intermittent fasting/‘time-restricted eating’, is a low-carb, Mediterranean-style diet, based on only 800 calories.
For some recent papers on intermittent fasting in the past year, see the following links:
Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting
Intermittent Fasting: Is the Wait Worth the Weight?
Compensatory Mechanisms Activated with Intermittent Energy Restriction: a Randomized Control Trial
Intermittent Fasting and Cardiovascular Disease: Current Evidence and Unresolved Questions
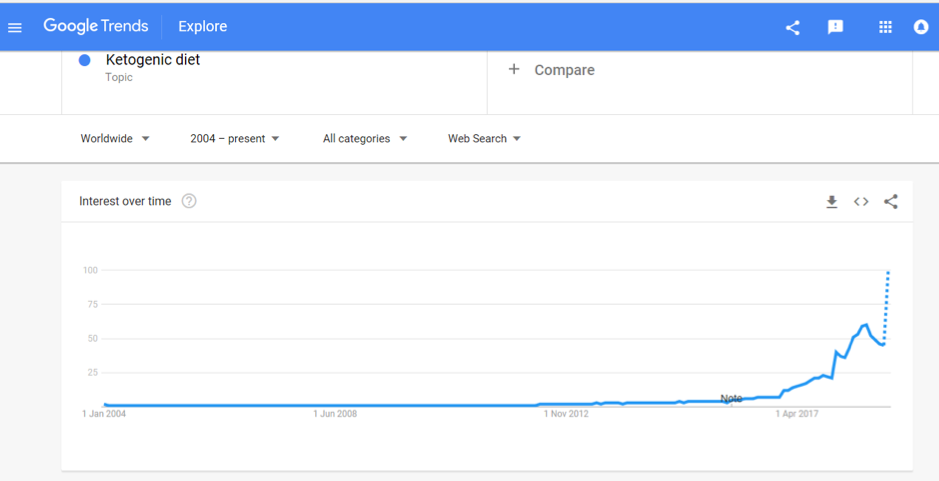
Veto keto
Also vying for the top spot of popular diets in 2019 is the Ketogenic Diet. A quick check of Google search trends shows that after bubbling away for the past few years, interest in this diet is starting to soar and it was the most searched diet term in 2018:

Being low-carb, high fat, the ‘traditional’ Keto Diet may jar against principles of plant-based eating, with new research in The Lancet reaffirming the importance of fibre (from vegetables and wholegrains) in the diet. Keto fans looking for a vegan or vegetarian version of the diet may instead opt for the plant-based version; dubbed ketotarianism, reminiscent of the pegan (paleo-vegan) that was also popular in 2018.
For some helpful papers on ketogenic diets published in the past year, see the following links:
A Nutritional Perspective of Ketogenic Diet in Cancer: A Narrative Review
A Systematic Review of the Use of Ketogenic Diets in Adult Patients with Cancer
The Ketogenic Diet in Disease and Development
Ketogenic Diet for Treatment of Intractable Epilepsy in Adults: A Meta-analysis of Observational Studies
Wellness woo
The Times has also just published an interesting article (which is unfortunately behind a paywall) which to sum up, provides (rather alarming) insight into what’s on the cards for ‘wellness revolutionaries’ in 2019; citing pink coconut water, quartz crystals, salt lamps, MCT oil, edible coffee bars and tongue-scraping, amongst other endeavours, all seemingly in the pursuit of health.
On the other hand, continuing to get good traction is the interest in digestive health and the microbiome, and plant-based eating, with Pinterest’s list of 100 emerging trends for 2019, reporting that searches for oat milk increased in popularity by 186% last year.
It is probably unfair to drop all these increasingly popular approaches into a fad bucket. Some, such as intermittent fasting, have a promising and growing evidence to their name and others may have snippets of beneficial principles in them, such as being plant-based, Mediterranean-style eating or with a focus on minimally processed foods.
Others, however, lack any credibly with regards to the claims they are making; often having inflated what is otherwise an incomplete evidence-base or simply just making things up.
In this era of ‘nutrition folk wisdom’, now more than ever is expertise needed from qualified dietitians and nutrition professionals to make sense of what is becoming an increasingly confusing dietary minefield.
Are there other trends that other dietitians or registered nutritionists do find helpful? Do let us know your thoughts. Or if you are a company and an organisation planning what trends you should support we are always happy to discuss and advise. Call us for a hello on 020 8455 2126 or email hello@mynutriweb.com
by Tanya HAFFNER | Jan 11, 2019 | The Nation’s Health
Happy New Year from the team here at Nutrilicious!
We thought that with the new year comes a great opportunity to take stock and consider what’s lined up for food, nutrition and public health in 2019.
Brexit: Politics and our plates
By far and away, the biggest thing in our diaries for 2019 will be Brexit and what will inevitably mark a fundamental change to the British food system as we’ve come to know it. Come 29 March, the deal will be done (or not!) and what that will look like is anybody’s guess right now.
The UK does not feed itself. We rely heavily on other countries for our food supply, with only 49 per cent of the food consumed in the UK produced here and 30 per cent coming from the EU; the equivalent to 10,000 shipping containers each day. For some commodities such as fruits and vegetables, our dependence on imports is much higher, in this case, we import 90 per cent of the fruits and vegetables we consume.
And so, because our food system is complexly intertwined with the EU, once we leave, it will significantly change our trading relationships, both with the EU, as well as those countries out of the EU that have trading agreements with it.
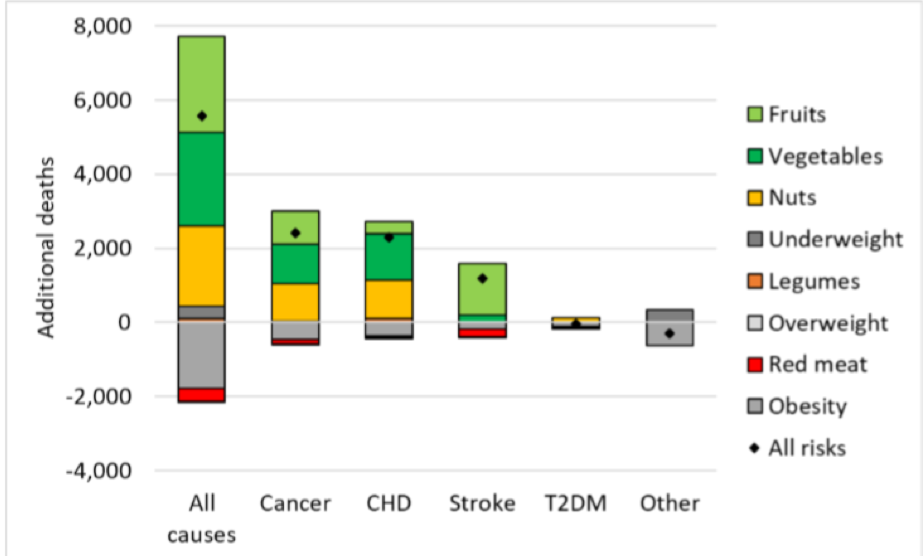
Consequently, people’s diets will be most likely be affected, with a working paper from the Oxford Martin School on the Future of Food warning that food prices are likely to increase, particularly for fruit and vegetables. According to this modelling, a Hard Brexit (trading on World Trade Organisation terms which imposes tariffs on imports) could lead to 5,600 additional deaths per year, associated with reduced consumption of fruits, vegetables, and nuts. This will not only affect individuals but the wider costs to society are pegged at increased healthcare expenditure at around 600 million GBP. On a positive note, there may be small benefits on obesity rates and reduced red meat consumption (see Figure 1)!

Figure 1. Changes in mortality in the UK by risk factor and cause of deaths under a Hard Brexit
The current deal on the table, due to be voted on in mid-January aims to provide a continuous tariff-free and quota-free access to EU markets, but even if voted through, the road ahead is likely to be tumultuous. Initially, the EU Withdrawal Act writes EU law over into UK law – triggering some necessary changes in relation to country of origin labelling and address information. Further changes to our food and nutrition labelling and food regulations may be unavoidable if international trade deals require them.
We should all be watching closely to how Brexit translates to the food on our table, dietary choices and ultimately public health.
For further information on how Brexit may affect the food system, we recommend reading the FRC’s Brexit briefing papers: https://foodresearch.org.uk/food-brexit-briefings/
EAT-Lancet Commission report
We’re expecting that the EAT-Lancet Commission report on Food, Planet, Health, due to launch on 17 January, is going to make waves. Never has the connection between food, planetary and human health been more apparent, with the need to address issues and impacts ever more pressing.
Housed at the Stockholm Resilience Centre, the EAT-Lancet Commission partnership brings together leading global researchers into five working groups, investigating:
- What is a healthy diet?
- What is a sustainable food system?
- What are the trends shaping diets today?
- Can we achieve healthy diets from sustainable food systems? How?
- What are the solutions and policies we can apply?
The report will include the latest research on each of these workstreams and will be publishing targets that deliver for both people and the planet.
For further information and to sign-up for updates, go to the Food, Planet, Health website: https://foodplanethealth.org
If you want to understand more about sustainable diets and how these new targets apply to your business, or would like a scientific review completed on another hot topic, please get in touch on 020 8455 2126.
Coming down the line from government
It looks like the team at Public Health England have been busy. While the rest of us were enjoying our mince pies, they have been working hard behind the sciences and they have kicked off the new year with the launch of new Change4Life messaging, raising awareness of the fact that on average, children are consuming their childhood sugar requirements by 10-years old.
But what else is on the agenda for the year ahead? With the updated Childhood Obesity Strategy published mid-2018 came promises of consultations on bans on pricing and positional promotions in retailers and a 9pm watershed for advertising of unhealthy food and drinks. Though we did see consultations conducted on the ban of sale of energy drinks to children and mandating calorie labelling in the out-of-home sector, some of the other consultations have not materialised yet, but they will be coming this year.
North of the border, the Scottish government also just completed their consultation on restricting junk food promotions, so it will be interesting to see what emerges there.
In 2018, SACN also consulted on their draft review of saturated fats, which recommended a continuation of previous COMA recommendations of 10% total calories. The final report is due at some point 2019 and is on the agenda for discussion at the next SACN meeting in March.
With saturated fat such a hot topic and matter of debate, keep your eyes peeled for this one, as it will provide some much-needed clarity and authoritative recommendations.
In addition, according to SACN meeting notes, the following items should also be expected in 2019:
- Whole Systems Obesity Programme: a joint initiative of PHE, the Local Government Association and the Association of Directors of Public Health are due to publish their guide and tools in the spring
- Product ranges targeted at babies and young children: scope and ambition for this programme is due mid-2019, following initial scoping and consultation that has already been conducted with industry and other stakeholders
- School Food Standards: technical update to commence in 2019
- National Diet and Nutrition Survey Year 1-9 Report: due imminently
So, that’s a brief flavour of some of the key things coming up on 2019. As ever, there’s lots of things to keep us busy!
Here at Nutrilicious we can help with your nutrition and health strategy, nutritional assessments of product portfolios, insights – views from the outside world of nutrition influencers and what they think of your offering – overall helping to put you on the front foot of your competition and upcoming government reformulation targets or standards. Or, perhaps you have key messages that you’d like to share with stakeholders through engaging new media such as interactive webinars and podcasts. To discuss your policy and communication requirements, you can reach us on 020 8455 2126.
Best wishes for a healthy and happy 2019.
by Tanya HAFFNER | Dec 13, 2018 | Thoughts
It’s that time of the year that many like to look back, take stock, share news from the past 12 months and look forward to what’s next.
We’re no exception.
We’ve done a lot of work that we’re extremely proud of in 2018. Today’s blog focuses on our NutriWebinars: launched less than a year ago and already a great success.
So what are they, why are we proud of them and how could you get involved (if you’re not already)?
What are NutriWebinars and how did they come about?
Well, as you’d expect, they’re webinars – or online seminars – to educate and train professionals about nutrition topics, aimed at the nutrition and food sectors.
They started because we’d experienced first-hand the many challenges in nutrition education and communications, including:
- The fast-paced environment;
- A requirement for Continuing Professional Development (CPD)
- Workers who are severely pressed for time, needing flexible opportunities to learn
- A desire from companies for convenient and cost-effective education and training solutions for their staff
In this digital age, webinars made simple sense to us.
They allow anyone to effectively engage with valuable information without having to be in the same physical place. Those who take part:
- Exchange opinions and experiences
- Get up-to-date content
- Interact with peers and colleagues online
- Receive online CPD certification
- Access slides and resources, delivered straight to their inbox
…all via a mobile platform, so you can access it wherever you are in the world.
‘Fabulous’ ‘Very informative’ ‘Highly recommend’
We tried them, refined them and they went down a storm: both with health professionals and, more recently, food sector professionals.
Topics have included calorie reduction, familial hypercholesterolaemia and sustainable diets.
Thousands of professionals who’ve joined us to learn and we’ve been overwhelmed with positive comments. ‘Highly recommend, with great CPD opportunities’, ‘fabulous’ and ‘very informative’ are just a few of the responses.
Our expert speakers love it too. As Professor Glenn Gibson summed his experience up, “I really enjoyed the NutriWebinar. The technology worked perfectly and this channel is such a fantastic way of communicating and avoiding all the crazy things we have to do these days to go and give talks, like travel for days for a one hour talk. Such a great team that held my hand to make it all run smoothly.”
We also worked with companies to deliver education and training to their staff using our full service platform. Our team includes experts in technology, healthcare, nutrition and digital marketing, so clients could choose their topic and leave us to do the work: facilitating registrations, devising and delivering content and all the administration.
With the technology easy to use and detailed reporting available, the webinars were hugely beneficial for organisations who value continuous analysis and improvement.
Where do we go from here?
It’s the end of the year and we’re celebrating our success, but of course we’re not resting on our laurels.
What’s next? Well, that in part comes down to you. We’ve got plenty of NutriWebinars planned but we’re also keen to hear from you about what topics you’d like us to cover.
Or, if you’re an organisation with training and education needs, we’d love to chat about how our platform can really deliver. Get in contact by email or via our online form
Follow us on Twitter: @NutriWebinar @Nutrilicious
Have a fantastic festive break and we look forward to seeing you in 2019!
by Tanya HAFFNER | Dec 7, 2018 | The Nation’s Health, Surveys and insights, Education
As Hippocrates, the father of modern medicine, said more than 2,000 years ago, ‘All disease begins in the gut’. And modern science is proving it as true today as it was then.
In this blog we outline the importance of gut microbiota and the use of diet to affect them to try to improve health and welfare.
For a detailed exploration of the topic, register for our free, CPD-accredited NutriWebinar. Led by experts Professor Glenn Gibson and Laura Tilt, it will give you both incredible insight into the science and practical tips on how to help balance gut microbiota for real health benefits.
The importance of the gut microbiome
We have more than 1,000 species of bacteria in our gut. And there’s been an increasing realisation among scientists that these can have a profound effect on our health – from Irritable Bowel Syndrome to infections, asthma and inflammatory disease right through to bone health and cognitive function.
This understanding has led researchers to investigate what we can do to affect the microbiota, to be applied to this wide range of health problems. A steady stream of scientific publications over the last 15 years address the topic, alongside research into probiotics and, more recently, prebiotics – which selectively fertilise the ‘good’ bacteria.
Our gut microbiome status changes throughout our lives. We acquire our gut bacteria mostly at birth. Moving through the milk years, there are differences in acquiring bacteria between breast-fed and infant formulae fed babies: human milk.
There is change again at the weaning stage, after which the gut microbiota remains fairly stable. As we get older there is then a decrease in the largely in beneficial bacteria like the bifidobacteria.
The gut microbiota can be susceptible to various challenges: stress, infection, antibiotics and poor diet all amongst the factor coming into play on a daily basis.
How does diet affect our gut microbiome and our health?
Carbohydrates, proteins, amino acids and lipids are all metabolised by microbiomes in different ways, with different outcomes for our health.
Carbohydrate metabolism – especially that of fibre – leads to organic acids, short chain fatty acids, that have shown to be beneficial in the gut. For example:
- Acetate is metabolised by the muscle, kidney, heart and brain
- Propionate, cleared by the liver, is an appetite regulator also said to be involved in cholesterol synthesis
- Butyrate is a fuel and regulates cell growth
Fibre itself can stimulate the growth of good bacteria. It’s been estimated that per 100g fibre fermented, 30g of bacteria is produced.
Metabolism of excess protein, on the other hand, leads to less positive end products:
- Ammonia induces quick cell turnover
- Phenols/indoles may act as co-carcinogens
- Amines are linked to migraine, cancer, schizophrenia
Balancing our gut microbiota
- Increased fibre intake
To help ensure balanced gut microbiota, our diet needs to include enough fibre. As discussed in our recent blog, government recommendations advise 30g per day for adults, representing a 60% increase in intake for most. Laura Tilt provides excellent advice on how this can be achieved in the NutriWebinar.
- Probiotic and prebiotics
Much work has been done into probiotic supplements: live ‘good’ bacteria that bring health benefits, especially lactobacilli and bifido bacteria.
More recently, scientists have found that prebiotics could have an even more profound effect on our health. They work by selectively proliferating beneficial bacteria, which in turn inhibit pathogens. They may also have a more general effect, including dampening inflammatory issues.
Prebiotics are found naturally in human breast milk and in fructans and inulins in vegetables including asparagus, onion, banana and leeks. They can also be taken as supplements, especially in GOS forms.
Takeaway message
As our understanding of the link between gut microbiota and our health has grown, researchers have increasingly looked to see where we can have the most impact.
We’re in a position where health and nutrition professionals can advise clients on what they can do to improve their gut health and therefore overall wellbeing. We look forward to our research widening and deepening further to improve our understanding in this vital area.
Get involved in the discussion on social media: @Nutrilicious @NutriWebinar #lifelonglearning #feedingthegut

 We’re excited to be part of the new initiative, Shop Well – Eat Well, to help enable this – especially targeting those on a low income.
We’re excited to be part of the new initiative, Shop Well – Eat Well, to help enable this – especially targeting those on a low income.